
Cub reporter, and Brown University student Dana Richie’s 6/22/23 article, “Did we need to be so isolated? Doctor critical of state’s response to Covid-19,” was a simulacrum of my May 13, 2023 evidence-based presentation at The Warwick Public Library. Richie ignored altogether the important validating first-person narrative contributions of my colleagues in medicine, oral surgery, law, teaching, small business, politics (i.e., state Rep. Michael Chippendale), radio media (i.e., WPRO’s Matt Allen), and journalism. The simplest way to demonstrate Ms. Richie’s warped shoddiness is to watch the various presentations oneself (here; here; here; here; here; here; here; here; here; here), and also view the slides I discussed (here). What follows is a formal written response.
Appropriately, Dana Richie rivets on my analysis (slides 5 & 6) of the joint Rhode Island Department of Health (RIDOH)-Brown University covid-19 hospitalization models, introduced by then Governor Gina Raimondo, during a live, nationally aired press conference (archived here), April 16, 2020. But Richie inappropriately writes that I “claimed,” or “according [to]” me those model projections were wildly inaccurate. Indeed, the models exaggerated actual covid-19-related hospitalizations (i.e., “with” covid-19, not necessarily because of covid-19; see slide 15, in particular) by > 6- to 12-fold, within 2- to 2.5-weeks of their public issuance. Those (see table, below) are hard data—from RIDOH/Brown University models, and RIDOH covid-19 hospitalization spreadsheet tallies (*re-accessed 6/24/23, per ongoing RIDOH revisions)—not mere “claims” on my part. No journalist, even a limited experience apprentice, or cub reporter, should employ such inaccurate language.

Dana Richie solicited “expert” rebuttal commentary from Mr. Joseph Wendelken (here; here), a RIDOH spokesman, and Dr. Stephen Buka, a Brown University epidemiologist. Mr. Wendelken has no training as a healthcare professional in medicine, or allied health, or epidemiology/public health. Wendelken’s training and background are in public relations and communications, and as a minor journalist (assistant Editor of the Queens Chronicle in New York City), after receiving an undergraduate degree at Providence College. Now an Adjunct Professor, Dr. Buka is a non-MD psychologist, with an Sc.D. in epidemiology, who specialized in the study of neuropsychiatric disorders. Buka has no publications whatsoever related to infectious disease, while there is no evidence he has ever designed and implemented any randomized, controlled trials, whether related to infectious diseases, or diseases pertaining to his own area of specific expertise, i.e., neuropsychiatric disorders. For my background, in contrast, see this curriculum vitae (circa 9/22), an amicus curiae brief (see p. 2) argued before the U.S. Supreme Court, and slides 2, 3, and 36.
Richie, introducing Mr. Wendelken’s initial “rebuttal,” again featuring her inaccurate, pejorative buzzword about my “claims,” wrote,
When informed of Bostom’s claims, Joseph Wendelken, Public Information officer for RIDOH, said that while in constant communication with hospitals, hospital leadership confirmed that at the time, hospitals “were indeed extremely stressed.” He added that all metrics the department used, including the hospital visit capacity and Emergency Department visits, indicated this as well.
Actual hospitalization and Emergency Department data from Rhode Island’s two largest hospital systems. Lifespan, and Care New England, put the lie to Mr. Wendelken’s unsupported contentions, as regurgitated uncritically by Richie. I presented the Lifespan hospitalization data during my lecture (see slide 7), and included an additional slide (38) on Lifespan Emergency Department visits, in the full slide presentation I shared with Richie. These data are summarized in a table below, compiled from Lifespan’s public annual reports, with the addition of data from a public Care New England 8/25/21 quarterly investor conference call presentation. The 8/25/21 Care New England presentation (on p. 15), illustrated directly below, even included a Venn-diagram slide, with the label “Bring Patients Back,” preceded by the explanatory comment, “Return (patient) volume to pre-covid levels”!
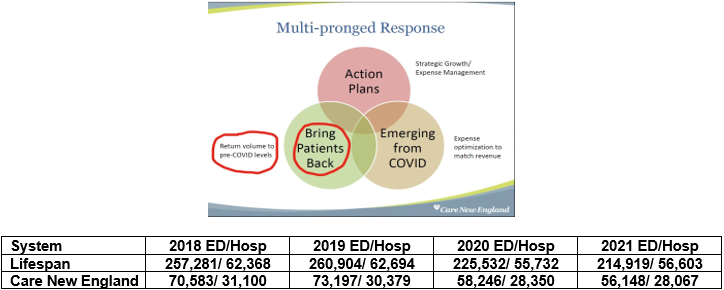
Debunking Mr. Wendelken’s anecdotal assertions, Lifespan experienced an ~10% reduction in hospitalizations, and ~15% fewer Emergency Department visits, comparing the pre-pandemic years of 2018 and 2019, to the covid-19 pandemic years of 2020, and 2021. For Care New England, those declines in the covid-19 years were ~8% for hospitalizations, and ~20% for Emergency Department visits.
Repeatedly, throughout my presentation, I referred to the “Swedish model” (citations provided; see slides 8, 17 and 39): no lockdowns, no imposition of mask mandates, and in-school face to face education throughout. Mr. Wendelken, who “disagreed with the Swedish model,” per Richie, stated without any reference (provided by Richie to back his claim), “during 2020, however, Sweden had 10X higher covid-19 death rates compared with neighboring Norway.” Wendelken’s unreferenced statement must be viewed in the larger, more complete context of these countervailing data:
—Unbiased total excess mortality data for Sweden during the pandemic (2020, through the end of 2022), by multiple estimates (here; here; here), place the country at or below all of its Nordic neighbors, and far below excess deaths in the U.S. This more meaningful outcome accounts not only for “covid deaths,” per se, but those deaths potentially related to “covid prevention” measures.
—So-called “covid-19 deaths” during the entirety of the pandemic (through June, 2023) were not “10X higher” in Sweden vs. Norway, rather they were ~2.3-fold higher. Comparable numbers vs. Denmark were ~1.6-fold , and Finland ~1.3-fold. Again despite these covid-19 numbers, no significant excess total mortality was observed in Sweden relative to these same neighboring countries.
—“Covid-19 deaths” were ~ 1.4-fold higher in the U.S. vs. Sweden, while total excess mortality in the U.S. during 2020-2022 (according to the Organization of Economic Cooperation, and expressed as a percentage increase) exceeded that of Sweden by ~8-fold! (i.e., 54.1% vs. 6.8%)
— Physician Preben Aavitsland, Director for Surveillance at the Norwegian Institute of Public Health, recently praised (English excerpts, here) Sweden’s covid-19 response, in particular its communication to the public. Dr, Aavitsland argued that other countries “hid their own insecurities by scolding Sweden,” because Sweden “undermined their mantra that we had no choice…We also have to look at how people’s physical and mental health has been affected, school results and drop-outs, unemployment and social economy and other things,” he said. He complimented the Swedish Public Health Agency’s communication over Norway’s, noting that it created less fear. “They gave more advice than threatened punishment.”
—Consistent with Dr. Aavitsland’s observations about “school results,” for example, open primary schools with teachers providing face-to-face education, and no masking throughout the covid-19 pandemic, were associated with “No learning loss in Sweden during the pandemic” vs. closed schools, “distance learning,” and mask mandates, in the U.S., yielding “historic learning setbacks for America’s children,” including Rhode Island schoolchildren.
Richie perseverated on her use of “claimed”/“claiming” when referring to hard data I presented (slide 23, with these Lancet “meta-analysis,” or best studies, “pooled” data for adults, and these N. Engl J Med data from ~900K U.S. children in North Carolina) that naturally-acquired immunity following SARS-CoV-2 infection was “more robust and enduring” for the prevention of serious covid-19 illness, than covid-19 vaccination (particularly mRNA vaccines). She also stated that I “argued”—not that I presented (slide 20) uniform, irrefragable randomized, controlled trial (RCT) data as aggregated by the pre-eminent arbiter of such RCT findings, The Cochrane Review, as well as two additional RCTs reported too late to be included in that Review—“that neither surgical nor N-95 masks are effective to prevent the spread of influenza or covid-19.” “Wendelken, “she then writes, “disagreed with these claims.” Again, absent any actual citations, Wendelken is quoted blandly asserting, “many studies have proven the efficacy of masking.” Furthermore, ignoring copious data I presented, especially RCT data, questioning covid-19 vaccine clinical efficacy and safety, including formal risk/benefit analyses, in low- to moderate clinical covid-19 risk populations (slides 25-30,citing these references, here; here; here; here; here; here; here; here; here; here; here; here; here), and Centers for Disease Control and Prevention (CDC) data [here; here] demonstrating that at least 55% of Rhode Island adults, and essentially 100% of Rhode Island children had been infected with SARS-CoV-2 by February, 2022, Richie quotes Wendelken stating, the vaccines “are safe and effective,” and “vaccine-induced immunity helps avoid the health risks associated with covid-19 infection.”
Dr. Stephen Buka, according to Richie, maintained “the state’s response followed infectious disease principles.” Dr. Buka, as I pointed out earlier, has no expertise in infectious diseases, nor does he apparently possess the curiosity to examine the historical responses to, and established public health recommendations for, respiratory viral pandemics. As I described during my presentation (slides 32,33) D. A Henderson, MD, MPH (d. 2016), was a Dean of the Johns Hopkins University School of Public Health from 1977 to 1990, and a leading figure in the World Health Organization’s successful smallpox eradication program, by ring vaccination. Perhaps Henderson’s very calm, sober perspective was shaped by dealing with a much more catastrophic illness—smallpox—which had a 20–60% fatality rate (persisting at 15-30% in its last endemic century), whose survivors were often maimed by the disease. This scourge, and the havoc it wrought, destroyed entire civilizations, and killed some 300 million in the 20th century, alone. As my lecture also documented (slide 9, citing these definitive references, here; here), the covid-19 infection fatality rate was only 0.1% among those <70-years-old, who comprise 94% of the world’s population, and even in the much higher covid-19 risk community dwelling elderly ≥ 70-years-old, rises to 2.9%—fatality rates vastly below those for smallpox.
In 2006, Dr. Henderson was the senior author on a seminal respiratory virus pandemic planning paper. Contra Dr. Buka’s uninformed assertions, here are the key res ipsa loquitur conclusions from Henderson and colleagues:
“There are no historical observations or scientific studies that support the confinement by quarantine of groups of possibly infected people for extended periods in order to slow the spread of influenza… The negative consequences of large-scale quarantine are so extreme (forced confinement of sick people with the well; restriction of movement of large populations)… that this mitigation measure should be eliminated from serious consideration… During seasonal influenza epidemics, public events with an expected large attendance have sometimes been cancelled or postponed, the rationale being to decrease the number of contacts with those who might be contagious. There are, however, no certain indications that these actions have had any definitive effect on the severity or duration of an epidemic… Schools are often closed for 1–2 weeks early in the development of seasonal community outbreaks of influenza primarily because of high absentee rates, especially in elementary schools, and because of illness among teachers. This would seem reasonable on practical grounds. However, to close schools for longer periods is not only impracticable but carries the possibility of a serious adverse outcome… In Asia during the (2003) SARS (-Cov-1) period, many people in the affected communities wore surgical masks when in public. But studies have shown that the ordinary surgical mask does little to prevent inhalation of small droplets bearing influenza virus. The pores in the mask become blocked by moisture from breathing, and the air stream simply diverts around the mask. There are few data available to support the efficacy of N95 or surgical masks outside a healthcare setting. N95 masks need to be fit-tested to be efficacious and are uncomfortable to wear for more than an hour or two… The problems in implementing such measures are formidable, and secondary effects of absenteeism and community disruption as well as possible adverse consequences, such as loss of public trust in government and stigmatization of quarantined people and groups, are likely to be considerable…Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted. Strong political and public health leadership to provide reassurance and to ensure that needed medical care services are provided are critical elements. If either is seen to be less than optimal, a manageable epidemic could move toward catastrophe.”
Dana Richie chose not to challenge Buka, or Wendelken on any of their counterfactual assertions. The now infamous RIDOH/Brown University covid-19 hospitalization models, for example, failed miserably in real time. Given their formal ties to RIDOH and Brown, at minimum, Wendelken and Buka should have been compelled to acknowledge those utterly failed models, openly, and honestly, and address why the draconian measures they begot were never reconsidered until months to years later! There were many healthcare clinicians and analysts, like me, who criticized, starting early in the spring of 2020, the policies Dr. Buka still champions. Our now validated criticisms, for which we were vilified by Buka’s ilk, were not as Buka falsely maintains, “after the fact,” and most assuredly not “easy” to proclaim.
I invite Mr. Wendelken and Dr. Buka to participate in a follow-up public seminar at The Warwick Public Library where we can cordially debate Rhode Island’s covid-19 response. Dana Richie is invited to attend this proposed event as well, and—hope springs eternal—cover the discussion in a much more informed, thoughtful, and objective manner.
Link to pdf of this essay: BLOG_Hard Objective Covid Data are Not “Claims”—Educating Cub Journalist Dana Richie
Link to pdf essay (edited, shorter version) slated to appear in The Warwick Beacon: Hard Covid Data are Not “Claims”—Educating Cub Journalist Dana Richie_900W
